
Dr. Nabeel H. Tammam FRCSEd. Consultant ENT surgeon
Definitions
Vertigo is an illusion of movement while dizziness means disequilibrium,
Faintness, giddiness, sensation of swimming or floating, unexpected falls,
anxiety or thinking difficulties in certain environments.
Benign Paroxysmal Positional Vertigo (BPPV) is a self-limiting vestibular
disorder, characterized by severe paroxysms of rotational vertigo provoked
by positional changes of the head. It may subside within a few weeks or
months, but can be chronic & severely incapacitating. Some patients
may experience remission & recurrences over time span of weeks to years.
Historical background
Prof. Robert Barany had been awarded the Nobel Prize for his work on the function of the vestibular apparatus. He described the condition of BPPV in 1921.
Physiological Aspects:
Functions of the vestibular system:
The vestibular system allows detection of the body motion in all three planes, consequent upon linear & angular acceleration stimuli applied to the head. In addition the vestibular system detects the gravitational vector, it is necessary for head & body orientations.
The vestibular system epithelium:
This is found in the three semicircular canals, utricle and saccula of each labyrinth. The sensory epithelium is localized to the maculae of the utricle, saccule & the cristae ampullares of the semicircular canals.
Macula:
Each macula is a small area of sensory epithelium. The ciliary bundles of the sensory cell project into the overlying statoconial membrane, which consists of an otoconial layer, a gelatinous area and a subcapsular meshwork. The otoconial layer comprises calcareous material, and the otocoie are of variable size.
Crista:
Each of the semi circular canals consists of an endolymph- filled canal with a dilated area (the ampula) in, which lies the cupula, which rests on the crista. The crista is surmounted by a bulbous, wedge-shape, gelatinous mass, the cupula. The cilia of the sensory cells project into the cupula.
Pathophysiology of the condition:
There are two theories behind it
A. Cupulolithiaisis :
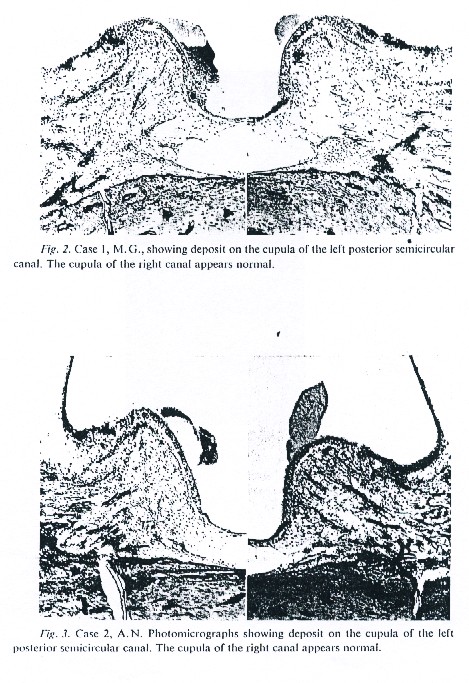
H.F Schukencht, in 1962 had proposed that a specific type of positional vertigo might be caused by detached utriclar otocoina, acting upon the cupula of the posterior semicircular canal.
In 1969, the pathological findings in the temporal bone of two patients, who exhibited this type of positional vertigo, were reported. It was shown that each had an inorganic deposit on the cupula of the posterior semicircular canal of the ear, which was under most in the provocative head position, and this disorder was termed “ Cupulolithiaisis”.
B. Canalithiasis:
John M Eply has advocated the canalithiasis hypothesis. Dense particles most likely displaced otoconia, collected in the most dependent position of the endolymph system, the long arm of the posterior semicircular canal.
A change in head position relatives to gravity causes the free canalliths to gravitate longitudinally through the canal.
These stimulate a leaky piston creating a hydrodynamic drag (downward force) in the canal.
After several seconds of latency required to overcome the inertia of the entire fluid loop in addition to cupular resistance, cupular displacement occurs, evoking sever nystagmus and vertigo.
When the cnaliths reach the limit of their descent, the drag ceases, bringing the nystagmus to an abrupt stop.
When the head maneuver is reversed, the particles gravitate in the opposite direction, producing nystagmus in the same axis but reversed in the direction of rotation.
On repetition of the head maneuver, the particles become dispersed and thus progressively less effective.
Diagnosis
There is a characteristic history of traumatic event to the labyrinth in the form of:
1- head injury
2- viral labyrinthitis
3- Surgical injury to the labyrinth.
4- Idiopathic
The disease is more common in female than male, age of 30-69 years (mean of 46 years)
The principal complains is sudden attacks of vertigo precipitated by certain head positions. The duration of each attacks lasts 5-10 seconds. The disease is self-limiting and subsides within few weeks or months. It recurs over times span of weeks to years. It is diagnosed by either positional test procedure (Dix & Hallpike 1952) or by modified Epley maneuver (1996).
The clinical forms
1- cute form :
Positional vertigo following head trauma. It improves or disappears
within months
2- chronic form :
Positional vertigo for a year or more
3- recurrent form:
Positional vertigo for weeks to months, separated by symptoms-free
intervals (months)
Treatment
The vestibular rehabilitation:
1- Brandt & Daroff exercises:
In 1980, Brandt & Daroff reported complete relief of symptoms in 66 of 67 patients with BPPV, as a result of precipitation head positions on repeated and serial basis.
The mechanism for this improvement was the proposed loosening and dispersion of otolithic debris from the cupula of the posterior semicircular canal, as a result of the rapid and aggressive vertigo-provocative movements.
2- Particle-repositioning procedure (PRP):
According to the canalithiasis theory, a single positional maneuver (Semont in 1988 and Epley in 1992) have been published. Which rely on the anatomical configuration of the posterior semicircular canal and the ability to reposition the head in verity of ways, to enable the offending debris in the posterior canal to migrate by gravitation via the common crus into the utricle.
Cooperative efficacy of various treatment of BPP
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Surgical treatment :
1- Singular Neurectomy by Gacek (1974):
The Singular nerve is the afferent part of the vestibular nerve, which arise form the hair cells of the posterior semicircular canal. Gacek proposed singular Neurectomy in 1974. It is indicated in chronic and recurrent forms.
A survey in 1981 was done among the member of the members of the American otological society, Whom had performed this kind of surgery. The result had showed that 96 surgeries done by 10 surgeon, 92% success rate in which their where relieve of the symptoms and 8% showed evidence of sensorineural deafness.
2- posterior canal occlusion by Parnes (1996):
The concept of the procedure based on the canalithiasis theory, the underlying cause of BPPV, so the blockage of the membranous duct eliminates endolymph movement within the canal, effectively fixing the cupula.
Parnes form Canada did ablation of the posterior semicircular canal
with stable hearing by brain stem evoked response audiometry on guinea
pigs, and that was the groundwork for the posterior canal occlusion procedure
to treat BPPV.
Parnes in 1990 first reported the success rate of this procedure on
2 human patients. The indications of this procedure are intractable cases
of BPPV and failure of vestibular rehabilitation (PRP)
Comparison efficacy of surgical treatment results.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
References
1. Dohlmen GF. Recollection of R.Baraney. Advance on otorhinolaryngology
1973;Vol 19 : XI-XIV .
2. Scott-Brown”s otolaryngology . Basic eciences.Fiifth edition, butter
worth & co (publisher ltd. , 1987 .
3. Sehuknecht HF, Ruby RRF. Cupulolithiasis Advances in otorhinolaryngology
1973: Vol.20: 434-443.
4. Epley JM. Particle repositioning for Benign Paroxysmal Vertigo.
Otolaryngology Clinics of North American 1996; Vol. 29, no 2: 323-331.
5. Luxon LM, Davies RA. Handbook of Vestibular Rehabilitation. Wharr
Publishers Ltd. London 1997;ch.3: 34-36.
6. Brandt T. Daroff RB. Physical Therapy for Benign Paroxysmal Positional
Vertigo. Archive of otolaryngology 1980:106: 484-485.
7. Eply JM. The Canalith repositioning procedure; for treatment of
Benign Positional Vertigo. Otolaryngology Head and Neck Surgery, 1992;
107:399404.
8. Semont A, Frenss G, Vitte E. Curring the BPPV with a laberetomy
Maneuver. Advances of Otorhinolaryngology 1988;Vol.42: 290-293.
9. Gacek RR. Pathophysiology and management of Cupulolithiasis Am.
J. otolaryngology, 1985:6:66-74.
10. Parnes lLS. Update on Posterior Canal Occlusion for Benign Paroxysmal
Positional Vertigo. Otolaryngologic Clinics of North America, 1996;Vol.29,
no.2: 33-342.